
In the beginning….
Up until the early 2000’s we labeled foot pain especially on the bottom of the heel as “plantar fasciitis”. The idea was the connective tissue (fascia) on the bottom of the foot was inflamed and causing pain due to overuse.
Because the thought process was plantar fascia was inflamed the treatments (and still the most common approach) was to decrease inflammation with ice, medications like NSAIDs and rest. When this didn’t work rest, orthotics, physical therapy to stretch the foot / calf and cortisone injections were then used.
The problem is these methods don’t work for the vast majority of people and studies show that over 50% of patients still have foot pain 15 years after it starts!
Let’s get updated on the research by Dr. Harvey Lemont
A study by Harvey Lemont, DPM, published in the May 2003 edition of the Journal of the American Podiatric Medical Association suggests that the term “plantar fasciosis” may be more appropriate than the commonly used “plantar fasciitis,” as biopsies reveal necrotic, or dead, tissue in the plantar fascia of people with this condition, not inflammation.
Lemont concluded that plantar fasciitis is a degenerative process, not an inflammatory process, involving small tears and tissue death in the plantar fascia—the thick band of connective tissue that spans and supports the foot arch—and intrinsic foot flexor muscles at their attachment on the calcaneus, or heel bone. Therapeutic efforts aimed at controlling inflammation, then, are often ineffective, as there is no inflammation present in the affected tissues.
IT’S A CIRCULATORY PROBLEM
- Entrapment of the posterior tibial artery by the flexor retinaculum—a fibrous band of tissue at the ankle under which various structures pass, including the posterior tibial artery—is one of the most likely causes of plantar fasciosis.
- Entrapment of the posterior tibial artery—the vessel that delivers blood to the plantar surface, or bottom, of the foot—may lead to decreased blood supply, tissue death, and pain in certain parts of the plantar fascia.
- Entrapment of the posterior tibial artery occurs when the big toe is held in an adducted (i.e., toward the midline of the foot) and extended position.
- In this configuration, the abductor hallucis muscle—the muscle that moves the big toe away from your foot’s midline—pulls on the flexor retinaculum and may restrict blood flow through the posterior tibial artery.
Problems with How your podiatrist treats foot pain:
Your podiatrist has 2 tools – Cortisone injections & Orthotics
Unfortunately most docs overlook and don’t have the time or the tools to provide a thorough examination and then effectively treat all of the contributors to foot pain. So instead they perform a simple cortisone injection and recommend orthotics to brace your foot. These are a generally bad idea.
Cortisone is known to degenerate tendons and ligaments. If you’re lucky you get 3 months of relief from a cortisone injection but nothing actually heals and you end up needing them regularly.
Orthotics make the 29 muscles that stabilize our foot weak. Now you have to wear weird shoes for the rest of your life and nothing ever got fixed. There’s a better way to treat foot pain. It involves a thorough physical exam and then a treatment that helps your body regenerate and heal itself.
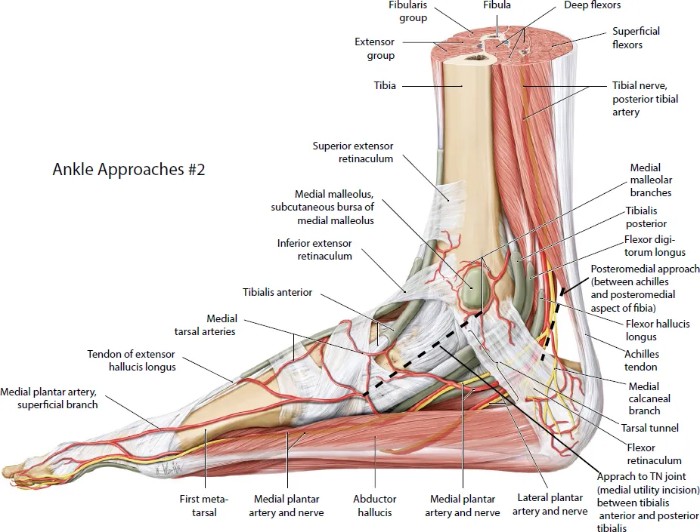
Anatomy overview of the Plantar Fascia and associated structures
Foot Muscles
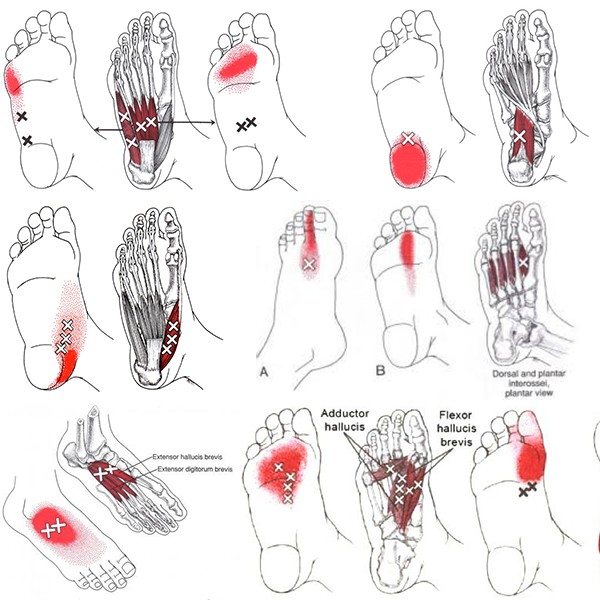
These are just some of the intrinsic foot muscles that don’t cross your ankle joint that can cause and contribute to your pain experience. I find that a good physical exam can help me to really zone in on the specific muscle that is causing your pain. I like to use a combination of dry needling and electro-acupuncture to release trigger points in these muscles and then change the chemical environment around those irritated muscles.
Nerve Pathways of the Plantar Fascia and bottom of Foot
Here’s the main culprits causing your pain. The Medial, Lateral Plantar Nerves, Medial Calcanal Nerve that all branch off of our Tibial Nerve.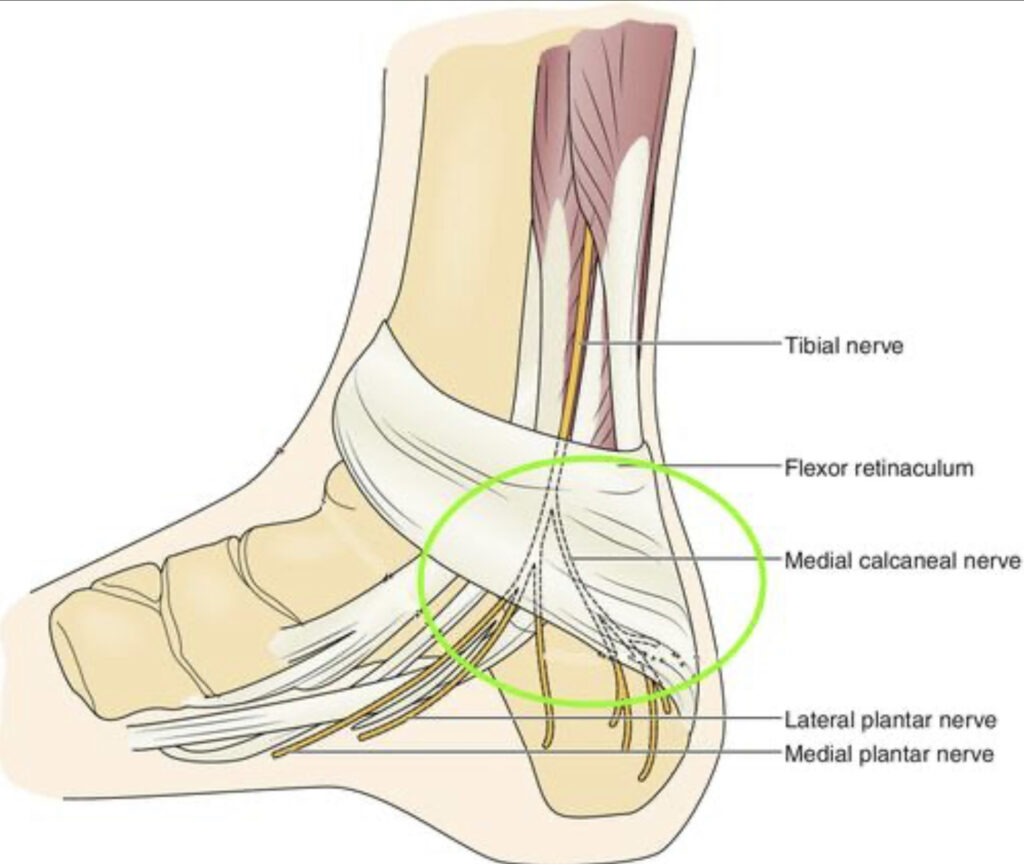
Both of these nerves start at the Ankle (by your Achilles’ tendon) and run down the bottom and sides of your foot. So if you have pain anywhere on your foot, that pain signal is coming directly from this nerve, to your spinal cord and then to your brain to get processed. When these nerves are irritated you will have pain.
The good news is that a number of specific techniques can addresses these irritated nerves – mainly neurofunctional Acupuncture & Perineural Injection Therapy with 5% dextrose.
Blood vessel pathways of bottom of foot
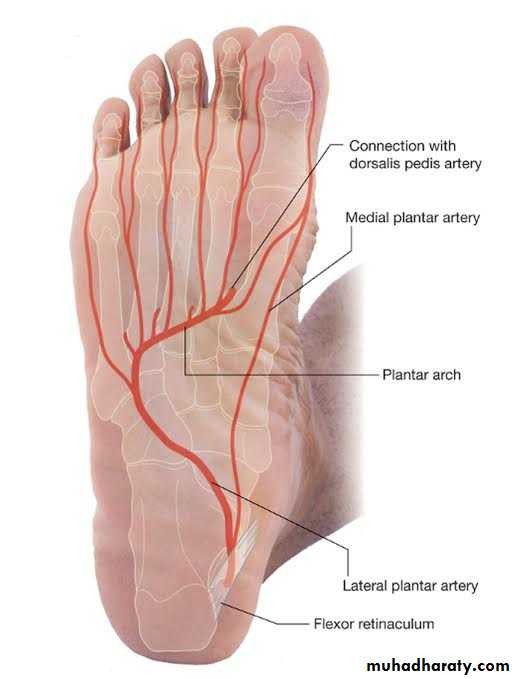
Posterior tibial artery divides to form the medial and lateral plantar arteries that broadly supply the sole of the foot. The medial and lateral plantar arteries supply the toes via the deep plantar arch.
A more effective treatment method
So we know that most foot pain isn’t inflammatory in nature and instead is a process of poor blood and nerve supply. So instead of rolling our feet on hard balls (further compressing tissue), icing (which reduces blood flow) or injecting steroids (which degenerate tissue) – we need to use treatments that bring blood flow, restore nerve function and help to regenerate degenerated tissue. The best tools for that are what Dr. Josh Hanson uses clinically every single day.
- Dry needling
- Neurofunctional Acupuncture
- Prolotherapy + Ozone (Prolozone)
What your foot pain comes down to…
- Poor blood supply
- Irritated nerves
- The inability of our cells to keep up with healing due to the 2 above factors.
If you’re sick of foot pain and are ready to take a more effective approach, don’t hesitate to reach out.
